The Democratic Republic of Congo is once again battling an Ebola outbreak, but this time health authorities are facing a particularly difficult challenge.
The virus is spreading through the country's conflict-ridden east, where insecurity, population displacement, weak healthcare infrastructure and the absence of an approved vaccine have complicated efforts to contain the disease.
Ebola, a highly infectious virus transmitted through close contact with infected individuals and bodily fluids, can cause severe hemorrhagic fever and has claimed more than 15,000 lives across Africa over the past five decades.
Experts warn that the latest outbreak could become one of the region's most difficult public health emergencies in recent years.
Congo officially declared its 17th Ebola outbreak on May 15, but evidence suggests the virus had been circulating for weeks, if not months, before authorities identified it.
Warning signs first emerged in early May when the World Health Organization received reports of a mysterious illness in the mining town of Mongbwalu.
Within days, four healthcare workers had died, raising concerns about a potentially serious outbreak.
Residents in Ituri province, the epicenter of the crisis, told reporters that unexplained deaths had been occurring since March. Rumors of a mysterious disease spread through communities long before medical officials confirmed Ebola as the cause.
Early detection efforts were hindered by the disease's symptoms, which closely resemble malaria, typhoid fever and yellow fever during its initial stages.
Several patients were initially misdiagnosed, allowing the virus to continue spreading unnoticed.
Laboratory challenges further delayed identification.
Testing facilities in Bunia, the provincial capital, were equipped primarily to detect the more common Zaire strain of Ebola and initially failed to identify the Bundibugyo strain responsible for the current outbreak.
By the time officials confirmed the disease, 246 suspected cases and 80 deaths had already been recorded across Ituri.
Concerns quickly extended beyond Congo's borders. On the same day the outbreak was declared, neighboring Uganda reported the death of a Congolese traveler linked to the outbreak, heightening fears of regional transmission.
Although Uganda has since confirmed only a limited number of cases, authorities moved swiftly to close border crossings and strengthen surveillance measures.
The rapid emergence of infections prompted the World Health Organization to declare a global health emergency, warning that the outbreak could persist for months if not aggressively contained. The Africa Centres for Disease Control and Prevention has also cautioned that as many as 10 countries could face elevated risk because of regional movement and trade routes.
One of the most troubling aspects of the outbreak is the strain involved.
The Bundibugyo strain currently circulating has no approved vaccine and no specific treatment, leaving health workers without one of the most effective tools used during previous Ebola outbreaks.
Vaccines developed during major outbreaks between 2018 and 2019 successfully targeted the Zaire strain but offer no protection against Bundibugyo.
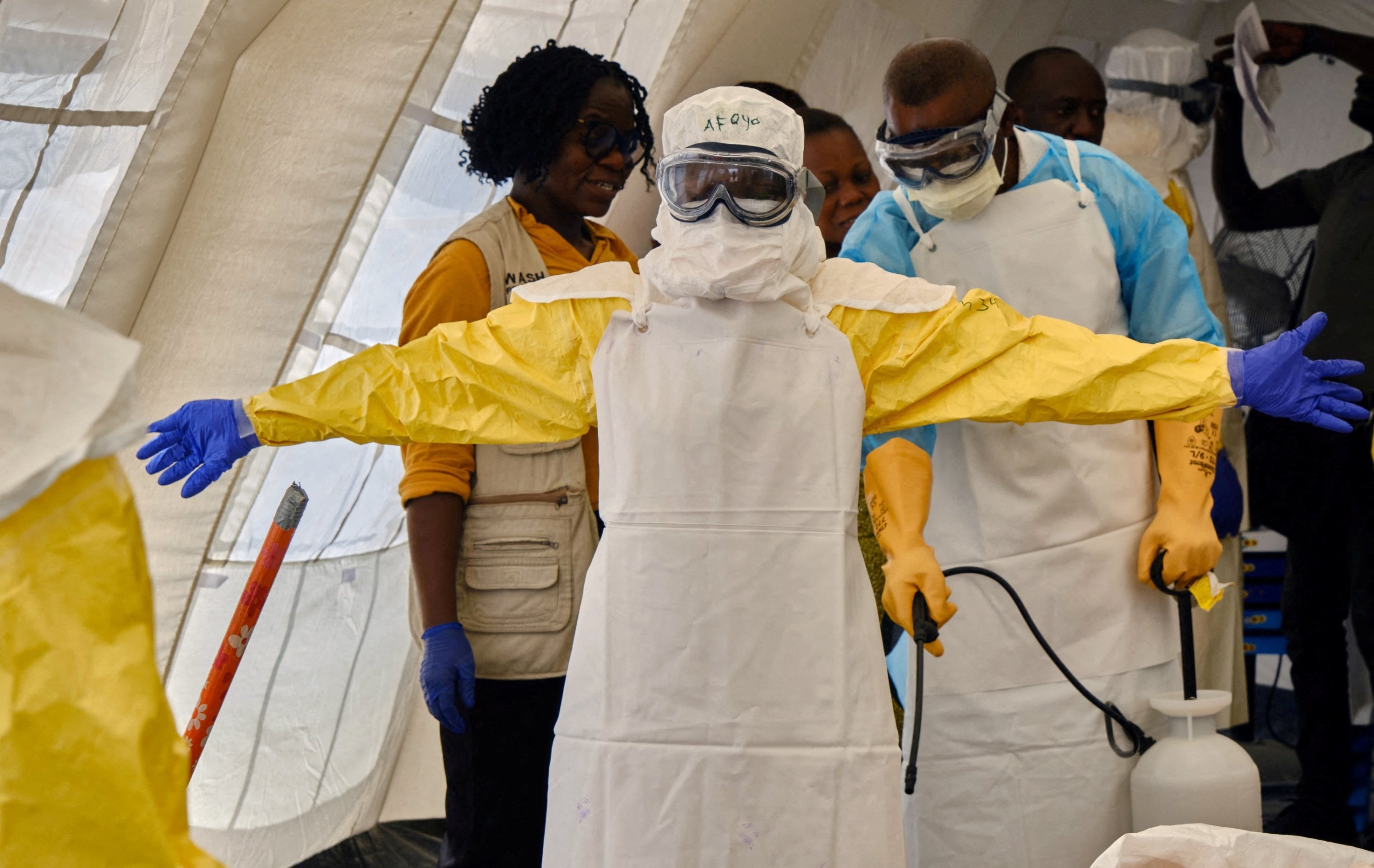
As a result, medical teams have been forced to rely on traditional containment strategies, including isolating infected patients, tracing contacts and educating communities. These methods can be effective but require rapid action, public cooperation and access to affected areas, all of which remain difficult in eastern Congo.
The disease itself presents additional obstacles. Early symptoms often resemble common tropical illnesses, delaying diagnosis and increasing the likelihood of further transmission.
Veteran Congolese virologist Jean-Jacques Muyembe, one of the scientists involved in the discovery of Ebola in 1976, acknowledged that the unusual presentation initially created confusion among medical professionals.
There is some hope on the horizon. Africa CDC says a vaccine specifically targeting the Bundibugyo strain could be available before the end of the year, with clinical trials under consideration. Until then, however, health workers must rely on conventional outbreak-control measures.
The outbreak is unfolding in one of the most unstable regions of the country.
Ituri has endured years of violence involving local militias and extremist groups, including factions linked to the Islamic State. Frequent attacks have displaced thousands of people, forcing families into crowded camps where infectious diseases can spread rapidly.
The insecurity has significantly hampered medical operations. Health workers often struggle to reach remote communities, while humanitarian organizations face logistical and security challenges when delivering aid.
The region's mining industry adds another layer of complexity. Constant movement of miners, traders and workers makes tracking infections and identifying contacts far more difficult than in more stable environments.
Healthcare facilities remain severely under-resourced. Many hospitals lack basic protective equipment and isolation facilities needed to safely manage Ebola patients.
In Bunia, patients displaying hemorrhagic symptoms have been seen arriving at hospitals on motorcycle taxis, often without adequate protective measures, increasing the risk of transmission.
Authorities also temporarily suspended flights to and from Bunia, a move intended to limit spread but one that also slowed the arrival of medical personnel and emergency supplies.
Aid organizations, including Doctors Without Borders, have criticized what they describe as a slow and fragmented response, warning that gaps in coordination could undermine containment efforts.
Beyond logistical and medical challenges, public mistrust remains a major concern.
In many communities across eastern Congo, years of conflict and limited government presence have weakened confidence in state institutions. As a result, some residents remain skeptical of official health guidance and continue to rely on traditional healers.
Health workers have encountered resistance in affected areas, making community outreach and disease surveillance more difficult.
There have also been reports of families attempting to remove the bodies of relatives who died from Ebola before proper burial procedures could be completed. Such actions significantly increase the risk of infection because the virus remains highly contagious after death.
Experts caution that the true scale of the outbreak may still be unknown. Limited testing capacity and restricted access to some communities raise concerns that additional cases have gone undetected.
With infections reported across multiple provinces and linked cases appearing in neighboring Uganda, regional authorities have introduced border closures, visa restrictions and other travel measures aimed at slowing transmission.
Despite the mounting challenges, health officials believe the outbreak can still be contained.
The Congolese government has rejected what it describes as overly alarmist assessments, maintaining that response efforts are gaining momentum and that the situation remains manageable.
Public health experts agree that containment remains possible, but success will depend heavily on improving community trust, expanding surveillance, strengthening healthcare resources and maintaining international support.
For now, traditional public health measures remain the primary line of defense against a virus that continues to exploit the vulnerabilities of a region already burdened by conflict and instability.
World Health Organization Director-General Tedros Adhanom Ghebreyesus recently expressed cautious confidence, saying that with sustained cooperation among governments, health agencies and local communities, the outbreak can ultimately be brought under control.